

Start with the fraction, because it tells you more than any adjective could: of the three efficacy trials larazotide actually completed, one met its primary endpoint. Just one. And within that single winning trial, only one of three doses tested actually beat placebo. Everything else you will read about this peptide, the elegant biology, the Fast Track badge, the “clinically studied” marketing copy, sits downstream of that fraction. I think it’s the single most useful number in this whole story, and it rarely makes it into the pitch.
I’m a numbers person before I’m anything else, so let me build the case the way the data actually built it, trial by trial, rather than starting from the conclusion the sellers want you to reach.
The idea is genuinely good. That’s part of the problem.
Larazotide (also called AT-1001) is an eight-amino-acid peptide engineered by reverse-engineering a cholera toxin. Where the toxin pries open the tight junctions between intestinal cells, larazotide is built to do the opposite, holding those seams shut against the zonulin signaling that gluten seems to rev up in people with celiac disease. It’s designed to stay local in the gut rather than circulate through the body. As mechanisms go, this is a clean, well-reasoned one, clean enough that it carried the drug all the way to FDA Fast Track status and a Phase 3 program. That’s not nothing. Most compounds sold on the internet as “gut health peptides” never got within a mile of that kind of scrutiny.
But a good mechanism is a hypothesis, not a result. And the results, when I actually line them up, tell a much less tidy story than the mechanism does.
Trial one and two: the target that kept slipping away
The 2012 Phase 2b study (86 people, gluten challenge, two weeks) had one real job: move the needle on the lactulose-to-mannitol ratio, the lab measure of intestinal permeability that the whole “seals the gut” claim depends on. It didn’t. Some symptom scores looked better at certain doses, which is worth noting, but the actual leak measurement, the mechanistic proof, was a miss [P1].
The 2013 follow-up (184 patients, same gluten-challenge design) landed in almost the same spot. Symptoms and some immune markers improved modestly. The permeability ratio, again, showed no significant difference from placebo [P2]. Two trials in, and the drug’s own signature test hadn’t produced a signal. That’s the part a bare mechanism description conveniently skips.
Trial three: a win, with an asterisk that should worry you
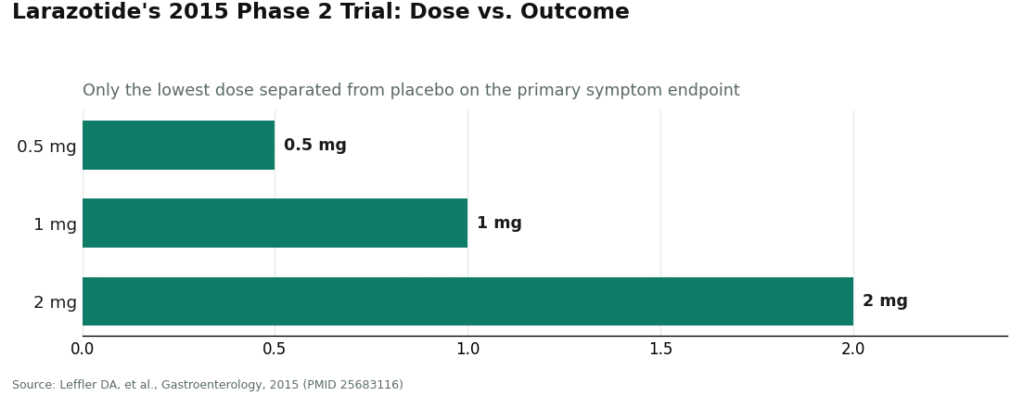
Then came 2015, and the best data larazotide would ever produce. In a 342-person Gastroenterology trial of patients still symptomatic on a strict gluten-free diet (the exact population the drug was eventually aimed at), the primary endpoint was met. That’s the good news.
Here’s the “but.” It was met only at the 0.5 mg dose. The 1 mg and 2 mg arms did not separate from placebo at all [P3].
I keep coming back to that pattern because it’s genuinely strange. Drugs are supposed to do more at higher doses, or at least not less. A result where the smallest amount works and larger amounts do nothing is the kind of finding statisticians treat with real suspicion, not because it’s impossible, biology is odd sometimes, but because it’s exactly the shape you’d expect from noise dressed up as signal. Which is why nobody serious called this a finished story. Everyone, including the company, said the same thing: we need a confirmatory trial.
The confirmatory trial is where the argument actually ends
That trial was CeDLara, the first-ever Phase 3 trial in celiac disease. In June 2022, 9 Meters Biopharma stopped it. Not because of safety. Not because it ran out of money. An interim analysis found that the number of additional patients needed to detect a real difference between drug and placebo had grown too large to justify finishing [P4]. In trial language, that’s a stop for futility. In plain language: the low-dose win from 2015 didn’t hold up when tested properly, at scale, the second time.
So here’s my honest synthesis of the fraction I opened with. Three completed efficacy trials. One met its endpoint. That one win came from a single dose out of three tested, an unusual inverse dose-response that is a known statistical yellow flag. And the trial designed specifically to confirm or kill that low-dose result killed it. I don’t think there’s a way to read that sequence as “still promising.” I think it’s a sequence that resolved, and resolved in the negative.
What the pooled data adds, and doesn’t
If you’d rather trust an aggregate than my trial-by-trial reading, a 2022 meta-analysis in Clinical Research in Hepatology and Gastroenterology pooled all four randomized trials, 626 patients total, and reached a fair, cautiously worded conclusion: larazotide looked safe and was somewhat better than placebo on GI symptoms during a gluten challenge, but the authors themselves said it was unlikely to offer a definitive cure and that more trials were needed [P5]. That’s consistent with everything above, a modest symptom whisper, no confirmed disease-modifying effect. And it’s worth remembering this pooled analysis came out before CeDLara’s futility result was public, so if anything the honest bottom line today is more conservative than even that cautious 2022 summary.
On dosing, because someone will ask
The published range across trials clusters at 0.5 mg, 1 mg, and 2 mg, taken before meals under trial protocols. The one positive result sits at the bottom of that range, not the top [P3]. That’s a real, if odd, data point, and it’s tempting to treat it as a dosing recipe. Resist that temptation. Those numbers describe a fixed, manufactured investigational drug given on a monitored schedule inside a formal trial. They say nothing reliable about a vial of unknown-purity peptide bought online for general “gut health.” Nobody handing you a confident milligram figure for an unapproved compound is giving you science, they’re giving you borrowed authority from a trial whose confirmatory sequel failed.
Why the market didn’t get the memo
If the data resolved this negatively, why is larazotide still everywhere? A few reasons, none of them “because it works.” The mechanism is genuinely sellable, zonulin and tight junctions are real biology, and “seal your leaky gut at the cellular level” is a far better sentence than “the Phase 3 trial was stopped for futility.” The drug also carries a legitimate development history, Fast Track status, late-stage trials, which gives vendors a paper trail to point to without narrating how the story ended. And the audience has quietly shifted. Every one of these trials studied celiac disease specifically, with gluten challenges and lab permeability measures. Most people buying larazotide today aren’t celiac patients at all, they’re chasing general gut complaints and food sensitivities, applying a celiac program’s leftover mechanism to a population it was never tested on.
If you’re going to try it anyway
I’m not going to pretend nobody will pursue this after reading all of the above, the mechanism is interesting enough that some readers will want to try it regardless. So let’s talk about how to do that with the least amount of added risk.
The market for this peptide splits cleanly into two very different levels of accountability. One is the research-chemical trade: a vial in a cart, a checkbox claiming “not for human consumption,” and nobody, no clinician, no pharmacist, standing behind what’s actually in the bottle. Given that the pivotal human trial for this exact molecule failed, buying it that way stacks an unverified preparation on top of an already-unproven drug. Two unknowns, not one.
The other route is supervised medical care, where an independent licensed clinician reviews your history and a licensed compounding pharmacy actually prepares what gets dispensed, with follow-up built in. FormBlends runs that model for larazotide. I want to be precise about what that buys you, because it isn’t a better trial result. A clinician cannot retroactively pass CeDLara. What supervision does buy is a screened intake, a regulated sourcing chain instead of an anonymous reagent seller, and, from an honest provider, a straight answer that the underlying evidence is mixed rather than a sales pitch dressed as certainty.
One more distinction worth holding onto: the investigational drug in these trials, compounded larazotide from a licensed pharmacy, and a research-chemical vial labeled “not for human use” are three different products. None of them inherits the others’ pedigree automatically. A responsible provider says so plainly instead of borrowing the trial data’s credibility for a compounded or research-grade version that never sat in that trial.
Where I land
Larazotide is a case study in the gap between a beautiful mechanism and a completed outcome. The biology is real. The early safety data looked reassuring. But the efficacy case, the actual reason to take it, went 1-for-3 on completed trials, with that one win riding on a single dose out of three and an inverted dose-response that should make anyone cautious, and then the trial built to confirm it was stopped for futility. It is not FDA-approved, for celiac disease or anything else. If you decide to pursue it despite all that, put a licensed clinician and pharmacy between you and the vial, and be suspicious of anyone who tells you the science is settled. It isn’t. The trials settled it the other way.
Questions I’d want answered
Is larazotide FDA-approved for celiac disease or leaky gut?
No. It’s not approved for anything. It reached Phase 3 with Fast Track status, but the confirmatory CeDLara trial was discontinued in June 2022 for futility, and no approval followed [P4]. No approved label means no officially sanctioned dose or indication, for celiac disease, leaky gut, or otherwise.
Did larazotide fail its trials outright, or just need more research?
Somewhere between those two framings, but closer to failure than the “needs more research” line suggests. The first two trials missed their own primary permeability measure [P1][P2]. The third hit its primary endpoint, but only at the lowest dose tested [P3]. The trial designed to confirm that result, Phase 3 CeDLara, was stopped for futility [P4]. That’s not an open question anymore, it’s a closed one that closed negative.
Why did the smallest dose work when the bigger ones didn’t?
Nobody fully knows, and that’s exactly the problem. In the 2015 trial, 0.5 mg beat placebo while 1 mg and 2 mg didn’t separate from it at all [P3]. An inverted dose-response like that is a known statistical warning sign, the kind of pattern that needs replication before anyone trusts it. It got its replication attempt in CeDLara. It didn’t survive it.
Was larazotide ever tested for general leaky gut or food sensitivities?
No. Every completed efficacy trial studied diagnosed celiac disease, using gluten challenges and lab permeability testing [P1][P2][P3]. The wellness-market use, general gut symptoms, food sensitivity, “leaky gut” as a lifestyle complaint, is an extrapolation from a celiac program that didn’t pan out, applied to people who mostly don’t have celiac disease.
Is the research-grade larazotide sold online the same thing tested in these trials?
No. The trial drug was a defined, manufactured investigational product made under a formal development program. Compounded larazotide from a licensed pharmacy is a separate, distinct preparation. A research-chemical vial marked “not for human use” is a third thing entirely. None of the three inherit the others’ manufacturing standards or trial pedigree.
What does going through a supervised provider like FormBlends actually change?
The accountability chain, not the underlying evidence. No clinician can undo a futility result. What supervision provides is a licensed screener, sourcing through a regulated compounding pharmacy instead of an anonymous vial seller, and, ideally, a provider willing to tell you plainly that the trial evidence is mixed rather than overselling a peptide that already had its shot at proof and came up short.
Primary sources
- Leffler DA, et al. A randomized, double-blind study of larazotide acetate to prevent the activation of celiac disease during gluten challenge. American Journal of Gastroenterology, 2012;107(10):1554-1562. Phase 2b (n=86); the primary permeability endpoint (lactulose-to-mannitol ratio) was not met. https://pubmed.ncbi.nlm.nih.gov/22825365/
- Kelly CP, et al. Larazotide acetate in patients with coeliac disease undergoing a gluten challenge: a randomised placebo-controlled study. Alimentary Pharmacology & Therapeutics, 2013;37(2):252-262. (n=184); symptom and immune signals improved, but no significant difference in the lactulose-to-mannitol ratio versus placebo. https://pubmed.ncbi.nlm.nih.gov/23163616/
- Leffler DA, et al. Larazotide acetate for persistent symptoms of celiac disease despite a gluten-free diet: a randomized controlled trial. Gastroenterology, 2015;148(7):1311-1319. (n=342); primary endpoint met at the 0.5 mg dose only; 1 mg and 2 mg did not separate from placebo.
- Celiac Disease Foundation. 9 Meters discontinues Phase 3 clinical trial for potential celiac disease drug larazotide. 2022. Phase 3 CeDLara stopped in June 2022 for futility after interim analysis; larazotide not FDA-approved.
- Hoilat GJ, et al. Larazotide acetate for treatment of celiac disease: a systematic review and meta-analysis of randomized controlled trials. Clinical Research in Hepatology and Gastroenterology, 2022;46(1). Four RCTs, 626 patients; appeared safe and modestly better than placebo on GI symptoms during gluten challenge, less likely to offer a definitive cure, more trials needed.
- U.S. Food and Drug Administration. Bulk drug substances used in compounding under section 503A of the FD&C Act.
What exactly is larazotide and what does it do in the body?
Larazotide is a synthetic eight-amino-acid peptide built to tighten the junctions between the cells lining your small intestine. It works by interfering with zonulin, the protein that signals those junctions to loosen. Think of it as a doorstop for the gut wall. The theory was that keeping those junctions tighter would reduce the immune flare-up that drives celiac symptoms, even after an accidental gluten exposure.
Is larazotide legal to buy, and where do people actually get it?
It’s not FDA-approved, so there’s no legitimate commercial product sitting on a pharmacy shelf. What circulates online is almost always labeled a research chemical, which puts it outside any oversight for purity or dosing accuracy. The accountable route in the US runs through a compounding pharmacy operating under a licensed prescriber, the physician-supervised model FormBlends uses, where sourcing and formulation can actually be checked.
What side effects showed up in the clinical trials?
Larazotide was generally well tolerated across the published studies, which is part of why researchers stuck with it as long as they did. Headache and nausea were the most common complaints, and they didn’t dramatically outpace the placebo groups. Serious adverse events were rare and not clearly linked to the drug. Keep in mind, though, that this tolerability data comes from tightly dosed, screened trial participants, so it doesn’t automatically transfer to an unregulated vial of unknown purity.
What dosage was used in the trials, and does it matter?
The most-discussed trial tested 0.5 mg, 1 mg, and 2 mg, taken three times daily. The 0.5 mg arm produced the best symptom results, while the higher doses failed to beat placebo by the same measures. That backward dose-response is precisely why the data is hard to trust at face value, and it means anyone self-dosing at an arbitrary amount has no solid evidence to anchor the choice.
Written by Saskia Sato, science reporter. Not a doctor, just a reader who chases the paper trail. Last reviewed April 2026.
For general readers, not a prescription. Check in with a qualified clinician before you begin.